
Posts by Skylar Pond
Lower Trapezius Band Press
T Spine Mobility
The Banded Sphynx is a strong thoracic extension stretch to get you from your office chair to the olympic platform.
Many of my patients are office worker by day/ athlete by night. After 8-10 hours in front of a monitor you’ll need a few quality mobility tools to replace that domestic slump with the triumphant T Spine extension you’ll need to catch weight overhead. Here are a couple of my favorites:
Grunt Big / Lift Big- Use your ventilation cycle to stiffen your spine.
From weightlifting and martial arts to opening a particularly tight pickle jar, when people attempt full exertion, the “grunt” is soon to follow. If you’re ever exercising in close proximity to a vigorous grunter you’ve probably wondered if this ritual is all together necessary.
The short answer is “yes”. Well maybe. They may just be obnoxious. I used to warm-up next to a man who would growl and caterwaul through hip rotations like a grizzly bear going through back labor. The grunt is not purely bluster though. If that weight room grunter is involved in a movement requiring optimal spinal stability, then that grunt is a valuable tool to prolong peak respiratory muscle contraction and stiffening of the spine.
In 2008 Wang and McGill studied the relationship between the muscles involved in respiration and their impact on spinal erector muscle recruitment. This study was published in Journal of Applied Biomechanics in 2008. This study of eight asymptomatic males without back pain revealed several interesting trends in the relationship between ventilation and spinal stability.
- With full inhalation the spinal stability increases
- The stability reaches to a maximum when the abdominal wall tightens to force air out of the lungs. The GRUNT occurs when you initiate the exhalation then quickly catch the breath and maintain peak spinal support of the respiratory muscles. It’s a clever and intuitive trick.
- That spinal stability decreases as air continues to leave the lungs
- Some individuals lose enough stiffness during the exhalation phase to compromise stability and are most vulnerable to injury during this phase of the ventilation cycle
Here are a couple practical applications:
1) If you or one of your athletes loses spinal stability during metcons, check if it is due to poor stabilizing motor patterns by placing the hands on the lateral abdomen above the iliac crests and checking for an ON/OFF pattern of the abdominal tone.
2) Attempt a challenging lower back stability move such as a one arm pushup or strict barrel roll during the exhalation phase. Try again while holding a deep inhalation and push into it. Go ahead and make some noise. If you notice a performance difference, use it when you need it.
Reading in Bed – Evening Magazine Clip
Hip Pain with Squat Cycles – An Old Country Salute to Anterior Hip Pain
There is nothing like a good squat cycle. After 3 to 6 grueling weeks under the bar, there is very little out there quite as rewarding as adding 5-20 pounds to a long standing 1RM. These gains however, do not come without a price:
1) Your new glute girth may ruin all of your dress pants at unpredictable and inconvenient times.
2) Your newly acquired posterior hip muscle strength may result in Anterior Hip Pain.
I’ve been working with strength athletes for many years. I am all too familiar with the sound of the athlete in my waiting room who is habitually and subconsciously thumping on their anterior hip with their own fist. This article will lay the groundwork for an effective preventative protocol as an alternative to that self percussive ritual now referred to as Old Country Sign.
Anterior hip pain is a common presentation for trainees undergoing a progressively loaded squat cycle. This pain is often blamed on a tight hip flexor and psoas. That is after all, the approximate location of the discomfort and the athlete does in fact present with a tight and painful psoas. The resulting advice is to stretch and rest the psoas but unfortunately, stretching and resting that tissue while continuing the progressive loading rarely results in symptomatic relief in any kind of timely manner. The reason that these stretches do not bring lasting relief is because they do not address the cause of the pain. The pain is likely the result of relatively weak hip flexors and rectus abdominis. Stretching and resting weak, inhibited tissues does not help them. The result of this relative anterior weakness is altered and aberrant motion in the hip socket and subsequent impingement. Allow me to explain.
The solution to this condition is balancing the forces which stabilize the hip and regaining optimal motion of that joint. This optimal motion is referred to as Joint Centration. A centrated joint is one which is supported proximally to distally, with balanced muscle forces across all angles of the joint. The result is that during the hip flexion of a squat, the head of the femur “spins” from the center of the acetabular joint without friction or impingement. (Picture a baseball spinning within the confines of an ice cream cone) The alternative is when the femoral head develops a tendency to “roll” instead of “spin” causing anterior motion within the hip joint. (Picture that baseball rolling up on and crushing the edges of that cone) This “rolling” results in the mechanical impingement and inflammation of the hip flexors and the presentation described by most symptomatic back squatters. The long-term chronic effect of this mechanical impingement is a self-perpetuating cycle where bony lesions form at the point of impingement as illustrated in the following video.
Clearly, the best course of action is to be proactive and to avoid the loss of joint centration that leads to this presentation. Your next question is “So what do I do?” Easy now. You’ll be better armed to manage your healthy hips over the course of your lifetime after I explain the mechanisms behind the exercises rather than if I were to turn you loose with a few new stretches.
Centration of the hip involves many tissues supporting a tremendous range of motion, but for this discussion on the squat, it will suffice to simplify into flexors and extensors of the lumbar spine and hip.
Posterior hip extensors:
Proximally attached- Glutes
Distally attached- Hams
Lumbar and Thoracic Spinal Extensors- Erector Spinae
Think about the muscles used during both the eccentric and concentric phases of the squat. These hip and spine extensor muscles are aggressively and preferentially strengthened during a squat cycle. To maintain pain-free hip motion, this shift toward extensor strength must be matched by trunk and hip flexor stability.
The posterior extensors of the glutes – and to a lesser extent, the smaller, deeper superior and inferior gemelli, are the tissues that require extra mobilizing and stretching to prevent their contraction from pushing and displacing the femoral head anteriorly into the front of the socket and the surrounding soft tissues. Don’t worry about stretching the hamstrings and the erector spinae as much for this presentation. Research (McGill Low Back Disorders 2nd Edition, 2007) has thoroughly demonstrated that lower back flexibility is more of a liability than an asset, so keep your mobility work for this condition focused on the glutes. Click Here for one of my favorite wall streches for the posterior hip/ glute/ piriformis/ gemelli.
Anterior Hip Flexors–
Proximally attached- Iliacus, Psoas
Distally attached- Quads, Rectus Femorus
Rectus Abdominus (particularly the lower portion)
Even with proper hamstring recruitment, the rectus femerus and other quadrucep muscles will be disproportionately strengthened in a squat cycle relative to the more important Short or Proximally insterted Psoas and illiacus. That means to avoid allowing your newly, powerful quads from turning your smoothly spinning bearing handle of a hip socket into a teeter totter, invest time into mobilizing the rectus femoris and strengthening and stabilizing the psoas and lower rectus abdominus.
OK. Finally. Let’s answer the question: “So what do I do to avoid anterior hip pain with squat cycles?”
1) Acute Phase- You are in a squat cycle and it is already symptomatic.
Once the symptoms have set in, you are best off icing, resting, getting soft tissue work, and stretching. Just do whatever you can to survive your squat cycle. The symptoms will not likely subside until the cycle is over and the inflammation runs its course. In extreme cases of discomfort or in chronically recurring cases, you will have to discontinue the squat cycle. Take that time to knock down the inflammation, retrain the anterior hip as described below, and then return to squatting with improved results.
2) Sub Acute- Proactive Phase- Stabilize and Balance Your Hips.
- Stretch- Gluteus Maximus, Rectus Femoris, Piriformis, and Gemellus
- Strengthen- Rectus Abdominus and iliopsoas. Strive to make gains in the static contractions as described below.
Pick several of these movements of appropriate challenge and train them year round. Your coach tells you to do extra pushups outside of your regular training right? Well here is one more reason to follow through on that advice. Ramp up the frequency of this skill work before squat cycles and attempt match the gains you make in your squat with equal gains in your static flexion endurance capacity.
Complimentary Hip Flexor and Rectus Abdominis movements:
basic-
- Plank and Pushup (Static)
- Inch Worm (Static)
- Mountain Climber (Dynamic)
- Heels to Heavens (Dynamic)
- Hollow Rocks and Hollow Robs (Static)
- Dead Bugs (Dynamic)
moderate-
- Toes To Bar (Dynamic)
- Knees to Elbows (Dynamic)
- Flutter Kicks (Dynamic)
- Ring Pushups (Static)
- Ring Pikes (Static)
- Ab Roll Outs/ AKA Ab Wheel/ AKA Evil Wheel (Dynamic)
advanced-
- Strict Renegade Rows (Static)
- Barrel Rolls (Static)
- Stir the Pot (Static)
- GHD Situp (Partial ROM)
- Front Lever (Static)
- L-Sit (Pull-Up, Ring Dip variations) (Static)
Pick a static movement of appropriate challenge and work to improve your max duration capacity to an equal proportion as your squat improvement. Integrate 2-3 dynamic movements into workouts, joint prep, or cool down per week.
The Big Picture:
When you undergo a cycle to increase the strength of your squat 1RM 10%, you must improve your plank by a comparable amount.
*Correcting hip centration is sometimes more complex than simply balancing the anterior side with the posterior side. If the above advice fails to yield results, make an appointment and have your firing patterns assessed to dial in your specific homework.
Standing Brugger Position
Here’s the Evening Magazine clip from 4/16/14. More to come. . .
Renegade Row
Stir the Pot
Barrel Roll Exercise
Simple Office Chair Stretch
Use this simple office chair stretch once per hour while seated at work. It has been demonstrated to objectively improve passive posture and you need only hold it for ten seconds.
Neck Injuries with Kettlebells? Fix Your Gaze / Fix Your Swing.
Neck Injuries with Kettlebells? Fix Your Gaze / Fix Your Swing.
Whatever modest success that I have had as a kettlebell competitor is due to the quality of my coaches. One of which is the current Guiness World Record holder for the hour long cycle and multiple Master of Sport in IKFF, the other is her coach, is the lead instructor for the Crossfit Kettlebell certification process and is an accomplished kettlebell athlete himself. If you find yourself lucky enough to receive their direct coaching and cues, do as you’re told. The results will follow. Their technique requires no external validation but I’ll provide it just the same.
Zach, Roo, their affiliate coaches and their interns teach the kettlebell swing as an integrated athletic movement. I will not endeavor to define the entire sequence. The purpose of this post is to explain one fact: We fix our gaze on a fixed point as we snatch and as we swing. Our necks are relaxed. The gaze is fixed on a single point allowing the torso and thoracic spine to rotate around it. The result is a smooth and subtle cervical extension at the bottom of the swing and a relative mild flexion at the lockout at the top of a kb snatch.
Here’s an example of the subtle cervical motion that I am describing. This short clip was taken at my last competition. This is how I was taught to move. Please notice that I fix my gaze on a spot on the floor about 8′ in front of me. Notice how I do not swing my gaze up and down with the bell as though I’m holding an orange or some other citrus fruit under my chin. I do not move my neck. Rather, my head is fixed and my body moves around me.
The reason that we move this way is simple and intuitive. We fix our gaze because it is the safest and most efficient way to move. Mild relative cervical motion occurs at the bottom of the swing for the same reason that a swimmer’s fixed neck rotates during a freestlye stroke relative to her rotating upper body. When you fix your gaze, you are not extending or moving your neck and head but relative extension does occur. A mildly extended neck position when not weight bearing is not dangerous or inefficient. It is a primal position hard wired into our neurology from our most primitive locomotor patterns. Watch a person move for the first time. What default cervical position does a baby adapt as it crawls?
The alternative to this relaxed and intuitive strategy is fixing the head as though holding a tennis ball under the chin and sweeping the head and gaze from floor to wall in each swing. This alternative approach is so stiff, unathletic and dysfunctional, that you need only try it to realize that it is a poorly thought out idea. Just for fun and to drive home the point, I’ll break down a brief argument into three categories: Safety, Performance, and Biomechanics.
Safety
The kettlebell swing is not a weight bearing neck exercise. It is an explosive hip movement. It is a jump where your feet never leave the ground. In the kettlebell swing the neck is not weight bearing. There is no more risk of a compressive extension injury while extending the neck a few degrees at the base of a kettlebell swing as there is looking up at a basketball before jumping for a rebound.
If you are recovering from a neck injury that is so inflamed that the mild relative motion involved in the proper mechanics of a swing is causing pain and inflammation, you need to put swings on the shelf for a couple weeks, get an assessment, some treatment, heal up and get back to the bell when you’re ready. It is better to peel back to a regression movement rather than defile your technique and stubbornly push through with stiff necked kettlebell swings.
Q- Ok it’s safe, but is fixing the gaze an effective way to stabilize and use the spine and has this been proven?
A- Yes it is. And Yes, it has.
Performance
Gabriele Wulf is a professor at the University of Nevada. She has published and impressive volume of studies over the past decade exploring the importance of fixing the gaze on an object and it’s effect on efficiency of movement and athletic performance. Her colleagues and she refer to it as “external fixation” or “attentional focus” and have proven time and time again that gaze fixation improves measureable markers of athletic performance in everything from muscular recruitment, to throwing darts, to juggling.
In 2007 she and her colleagues analyzed in a published controlled study the effect of fixing the gaze upon a target in the vertical jump test. As I described before, the hip extension of a kb swing or snatch closely matches that of the mechanics of a vertical jump. This is as good a study as we can ever hope to find on this topic. In fact it exceeds the expectation that I had when I began researching this article. In her study, she had uninstructed control groups to simply jump as high as they were able using whatever strategy they felt was most effective. Those participants were then instructed to fix their gaze upon the vertical target (mild cervical extension and gaze fixation- sounds familiar right?) and attempt again. Their vertical jump and center of mass height improved measurably and significantly (1.0 cm improvement on average) compared to controls. If you have the time, please read the linked out studies. The case is closed on performance. Thanks for playing. We could skip to my a conclusion from here, but I’ve got one more thing on my mind so bear with me for another paragraph or two.
Biomechanics
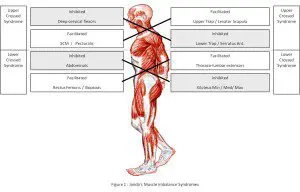
Some have mistakenly referenced the Joint By Joint model of movement to rationalize striving for a fixed neck/ cervical region. The Joint by joint model is adapted from Janda’s Layer Syndrome as pictured below. It describes a common biomechanical fault of stiff/ hypertonic neck and upper back. This is not an ideal to be aspired for. This is a pathological presentation. These stable/hypertonic areas require mobility. When these imbalances or not addressed, the result is the Upper and Lower Crossed Syndromes also pictured below. These models, when understood and applied correctly, would actually support increased cervical mobility which is achieved with the fixed gaze, mobile cervical style of swing as taught by my coaches and most of the serious coaches in the kettlebell world.
In fact, fixing the treatment area and creating relative motion at that segment by moving the body around it is often THE most effective way to rehabilitate, activate and treat the neck. Examples of this style of mobility include the Turkish Get-Up and Baby Get-Up for shoulder and glute medius rehabilitation. The days of clam shell exercises and banded external rotation exercises are behind us. If corrective exercise is to have a lasting effect, it must be integrated and functional.
Conclusion:
Holding a tennis ball, large orange or grapefruit under your chin while exercising is not entirely useless. Grapefruit is high in citrus bioflavonoids which help in the healing process and will prevent scurvy. If you are holding a grapefruit under your chin while you kettlebell, please remove it and eat it. Don’t worry about “breaking your canister” by fixing your gaze. Athletes’ necks move when they kettlebell swing, when they swim, and when they jump. Attempting to swing your gaze from the floor to the wall with a stiff neck will not make you safe, nor will it make you effective. When you swing a bell, lock your spine into a rigid lever, fire your hips into extension, and allow your neck to relax and respond naturally.
About the Author:
Dr. Pond holds the rank of IKFF Elite Level Sprinter which he earned at this year’s Northwest Kettlebell Championships in the #70 snatch division.
#poohjacked
This repost is brought to you by the Blog of Morgan Junction Crossfit– Old Country Strong
“Winnie The Pooh is JACKED.”

– Well worn poohbook
I’ve read my boys our A.A. Milne copy of Pooh so many times that the hard cover was lost and forgotten years ago. I’ve always been fond of the bear of very little brain, but this was an angle I had not yet considered.
This all started with the Zach Filer’s random and passionate assertion that “Grizzley bears eat honey for strength.” It then got personal – “Winnie the Pooh is JACKED. YOU need to get #poohjacked.” Yes, he sometimes hashtags verbally. This came a little out of left field but he was armed with the swift and blinding logic of a man used to arguing his point.
1) “The man has no neck”
2) “His arms are as thick as his quads!”
3) “He doesn’t have thumbs so he carries shit with a Gorilla Grip all day long.”
The guy is starting to make a lot of sense here. I looked over my old book with new eyes and came to the following conclusion:
I do need to get Poohjacked, and you do too.
First off, let’s get real clear about which Winnie The Pooh we’re talking about here. The original 1926 Pooh is the only jacked one. This is an important distinction and it may prove useful.
Exhibit A – JACKED

– A thumbless Gorilla grip farmers’ carry all day long without a stitch of clothing on. The guy is a legend.
Exhibit B – Distinctly NOT JACKED

– Rounded Thoracic spine to match some anterior head carriage. Shame. Oh, and Sweet midriff.
Never mind the fact that the Disney bear or Exhibit B has so habitually broken his gorilla grip that he actually grew thumbs. The important distinction between the two and the secret to the original Pooh’s stoutness is his rigid spine. He is a stuffed bear and likely has no spine so he has that genetic advantage but you could learn from this bear of very little brain.
Maintaining a rigid spine during athletic movements allows the athlete to treat their spine and surrounding musculature like an efficient and simple system of levers and pullys. The ability to maintain rigid tension through that lever determines how much energy is wasted in the motion between the 26 individual elements that compose the lever that is your spine.
Countless other examples of #Poohjacked can be found.

– Rigid spine = Perfect hamstring tension while dislodging one’s self from pots of hunny.

– No spine means no problem knocking out hollow rocks and long sets of perfect push-ups while hitting that morning session of “stoutness exercises before the glass.”

Need to hold plank while you check if a heffelump has eaten your honey in the bottom of a Very Deep Pit? Not a problem.
Conclusion: Life is hard when you have a spine. Everything from hamstring tension to your workplace ergonomics wants to flex your spine and compromise that powerful lever that you work so hard to maintain. The explosive hip extension that you cultivate as an athlete is a canon. If your spine lacks the capacity to lock into rigidity, then you are firing the canon from a canoe. Every time you pick something up, every time you sit down, you have a choice. Build a barge. #poohjacked
Written by: Skylar
About the Authour: Dr. Skylar Pond graduated from The University of Western States with a doctorate in chiropractic in 2008. He continued his education at UWS to achieve the additional degree of Certified Chiropractic Sports Physican and serves as the team physician of the Old Country Iron Club’s Competition Team. To fully view Sky’s background and look at his home facilities web page Click Here to learn more about the Doc.